
Understanding Percutaneous Augmentation and Annuloplasty
Percutaneous Augmentation is a medical procedure that is minimally invasive and used to reinforce or strengthen a structure within the body without requiring open surgery. This technique typically involves using percutaneous (through the skin) techniques to support or augment a body part or structure.
On the other hand, Annuloplasty is a surgical procedure that aims to repair or reconstruct a ring-like structure, such as the fibrous ring of a heart valve. This procedure is commonly performed to treat conditions like valve regurgitation (leakage) or to restore proper function to a valve that has become enlarged or distorted.
When the two procedures are combined, Percutaneous Augmentation and Annuloplasty may describe a minimally invasive procedure used to reinforce or repair a ring-like structure within the body. For instance, it may involve using minimally invasive techniques to support or modify the fibrous ring of a heart valve without the need for open-heart surgery. This reduces the invasiveness of the procedure and potentially shortens the recovery time for the patient.
Percutaneous Augmentation and Annuloplasty (22526-22527)
22526: Percutaneous intradiscal electrothermal annuloplasty, unilateral or bilateral including fluoroscopic guidance; single level
22527: Percutaneous intradiscal electrothermal annuloplasty, unilateral or bilateral including fluoroscopic guidance; one or more additional levels
Intra-discal procedures are minimally invasive surgical procedures. These procedures involve the insertion of an intra-discal probe into the problematic disc(s). Through the use of radiofrequency or electro-thermal energy, heat is produced to decompress the disc material by coagulating and shrinking type I collagen in the disc (TIPs).
Another method is the injection of agents into the nucleus pulposus or annulus of the disc to decompress the disc material. There are also percutaneous procedures that use indirect or direct visualization to decompress the disc material.
The purpose of intra-discal procedures is to treat patients with discogenic pain that is caused by annular disruption of a contained herniated disc. These procedures aim to seal annular tears or fissures, destroy nociceptors, or relieve pain.
Thermal intradiscal techniques use single or multiple probes/catheters that utilize a resistance coil or other delivery system technology. These probes can be flexible or rigid and are placed within the nucleus pulposus, the nuclear-annular junction, or within the annulus.
Intradiscal procedures are medical procedures that involve treating the spine by accessing the discs that are found between the vertebrae. The procedures include a variety of techniques that aim to alleviate pain and discomfort caused by spinal disorders.
Some common examples of intradiscal procedures include annulo-nucleoplasty (also known as the Disc-FX procedure), cervical intradiscal radiofrequency lesioning, coblation percutaneous disc decompression, intradiscal biacuplasty (IDB), intradiscal electrothermal annuloplasty (IEA), intradiscal electrothermal therapy (IDET), intradiscal thermal annuloplasty (IDTA), nucleoplasty (also known as percutaneous radiofrequency thermomodulation or percutaneous plasma discectomy), percutaneous (or plasma) disc decompression (PDD), percutaneous intradiscal radiofrequency thermocoagulation (PIRFT), radiofrequency annuloplasty (RA), and targeted disc decompression (TDD).
Additionally, intradiscal injections may also be used as a treatment option for some conditions. These injections may involve substances such as methylene blue, hyaluronate, ozone, oxygen/ozone, bone marrow concentrate, chymopapain, platelet-rich plasma (PRP), mesenchymal stem cells, glucocorticoids, hyaluronidase, growth factors, and more.
Arthrodesis (22532-22819):
Arthrodesis is a surgical procedure that may be performed alone or in combination with other definitive procedures such as osteotomy, fracture care, vertebral corpectomy, or laminectomy. When arthrodesis is performed along with another definitive procedure, modifier 51 is appropriate. However, arthrodesis codes 22585, 22614, and 22632 are add-on procedure codes and should not be used with modifier 51. To report instrumentation procedures, see 22840-22855, 22859. Codes 22840-22848, 22853, 22854, and 22859 are reported along with code[s] for the definitive procedure[s]. If instrumentation reinsertion or removal is performed with other definitive procedures, including arthrodesis, decompression, and exploration of fusion, append modifier 51 to 22849, 22850, 22852, and 22855. To report the exploration of fusion, use 22830.
If exploration is performed with other definitive procedures, including arthrodesis and decompression, append modifier 51 to 22830. Do not append modifier 62 to spinal instrumentation codes 22840-22848, 22850, 22852, 22853, 22854, 22859. To report bone graft procedures, see 20930-20938. Report bone graft procedures in addition to code[s] for the definitive procedure[s]. Do not append modifier 62 to bone graft codes 20900-20938.
Lateral Extracavitary Approach Technique
22532 Arthrodesis, lateral extra cavitary technique, including minimal discectomy to prepare interspace (other than for decompression); thoracic
22533 Arthrodesis, lateral extra cavitary technique, including minimal discectomy to prepare interspace (other than for decompression); lumbar
✚ 22534 Arthrodesis, lateral extra cavitary technique, including minimal discectomy to prepare interspace (other than for decompression); thoracic or lumbar, each additional vertebral segment (List separately in addition to code for primary procedure)
Here’s an example of a medical case involving the use of CPT code 22532:
Patient Information:
- Name: Sarah M.
- Age: 45
- Medical History: Sarah has had a history of chronic lower back pain for the past six years. MRI scans revealed degenerative changes in the L4-L5 vertebrae, causing severe spinal instability and persistent discomfort.
Presenting Symptoms: Sarah experienced excruciating lower back pain radiating down her left leg. She had difficulty standing for extended periods and noticed progressive weakness in her left leg.
Pre-operative Evaluation: Upon consultation with a spine specialist, Sarah underwent various assessments, including neurological examinations and imaging studies. MRI and CT scans revealed disc degeneration and spondylolisthesis at L4-L5, confirming the need for surgical intervention.
Surgical Procedure: Sarah underwent a posterior lumbar fusion (CPT code 22532) to stabilize the affected segment. The surgical team employed a posterior approach, using pedicle screws and rods to fuse the L4 and L5 vertebrae.
Post-operative Care: Sarah was closely monitored in the hospital for four days post-surgery. Physical therapy sessions commenced immediately to aid in her recovery and to regain strength and mobility.
Outcome:
- Short-Term: Sarah reported a significant reduction in back pain post-surgery. Her leg weakness also improved gradually during her hospital stay.
- Long-Term: Over the following months, Sarah continued physical therapy and gradually resumed daily activities. At the one-year follow-up, she reported minimal discomfort, improved mobility, and a significantly enhanced quality of life.
Conclusion: The case of Sarah M. demonstrates the successful application of CPT code 22532, where a posterior lumbar fusion effectively addressed severe spinal instability and chronic pain, leading to substantial improvements in function and overall well-being.
Anterior or Anterolateral Approach Technique
Procedure codes 22554-22558 are for SINGLE interspaces; for additional interspaces, use 22585. A vertebral interspace is a non-bony compartment between two adjacent vertebral bodies, which contains the intervertebral disc and includes the nucleus pulposus, annulus fibrosus, and two cartilaginous endplates.
For the following codes, when two surgeons work together as primary surgeons performing distinct part(s) of an anterior interbody arthrodesis, each surgeon should report his/her distinct operative work by appending modifier 62 to the procedure code.
In this situation, modifier 62 may be appended to the procedure code(s) 22548-22558 and, as appropriate, to the associated additional interspace add-on code 22585 as long as both surgeons continue to work together as primary surgeons.
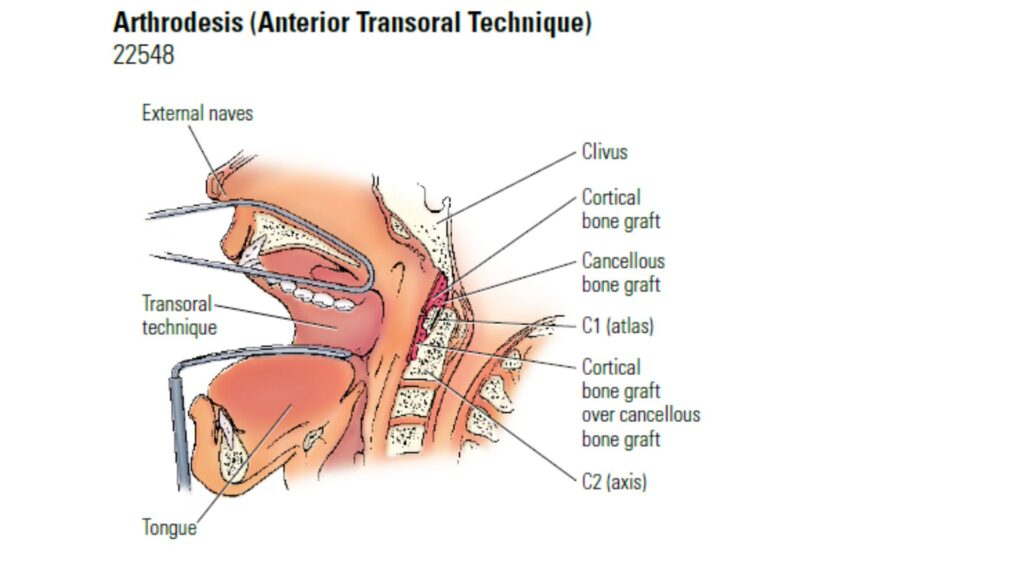
22548 Arthrodesis, anterior transoral or extraoral technique, clivus-C1-C2 (atlas-axis), with or without excision of the odontoid process
(For intervertebral disc excision by laminotomy or laminectomy, see 63020-63042)
22551 Arthrodesis, anterior interbody, including disc space preparation, discectomy, osteophytectomy, and decompression of spinal cord and/or nerve roots; cervical below C2
✚ 22552 cervical below C2, each additional interspace (List separately in addition to code for primary procedure)
(Use 22552 in conjunction with 22551)
22554 Arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression); cervical below C2
22556 Arthrodesis, anterior interbody technique, including minimal discectomy to prepare interspace (other than for decompression); thoracic
Do not report 22554 and 63075 together, even if done by different people. Use 22551 for reporting anterior cervical discectomy and interbody fusion at the same level during the same session.
Thank you for Visiting to Health Coding Hub
For any queries, please reach out to us at info@healthcodinghub.com